The 7 Extraocular Muscles
4 Rectus Muscles
Superior rectus
Inferior rectus
Medial rectus
Lateral rectus
2 Oblique Muscles
Superior oblique
Inferior oblique
1 Eyelid Muscle
Levator palpebrae superioris
Extraocular Muscle Origins
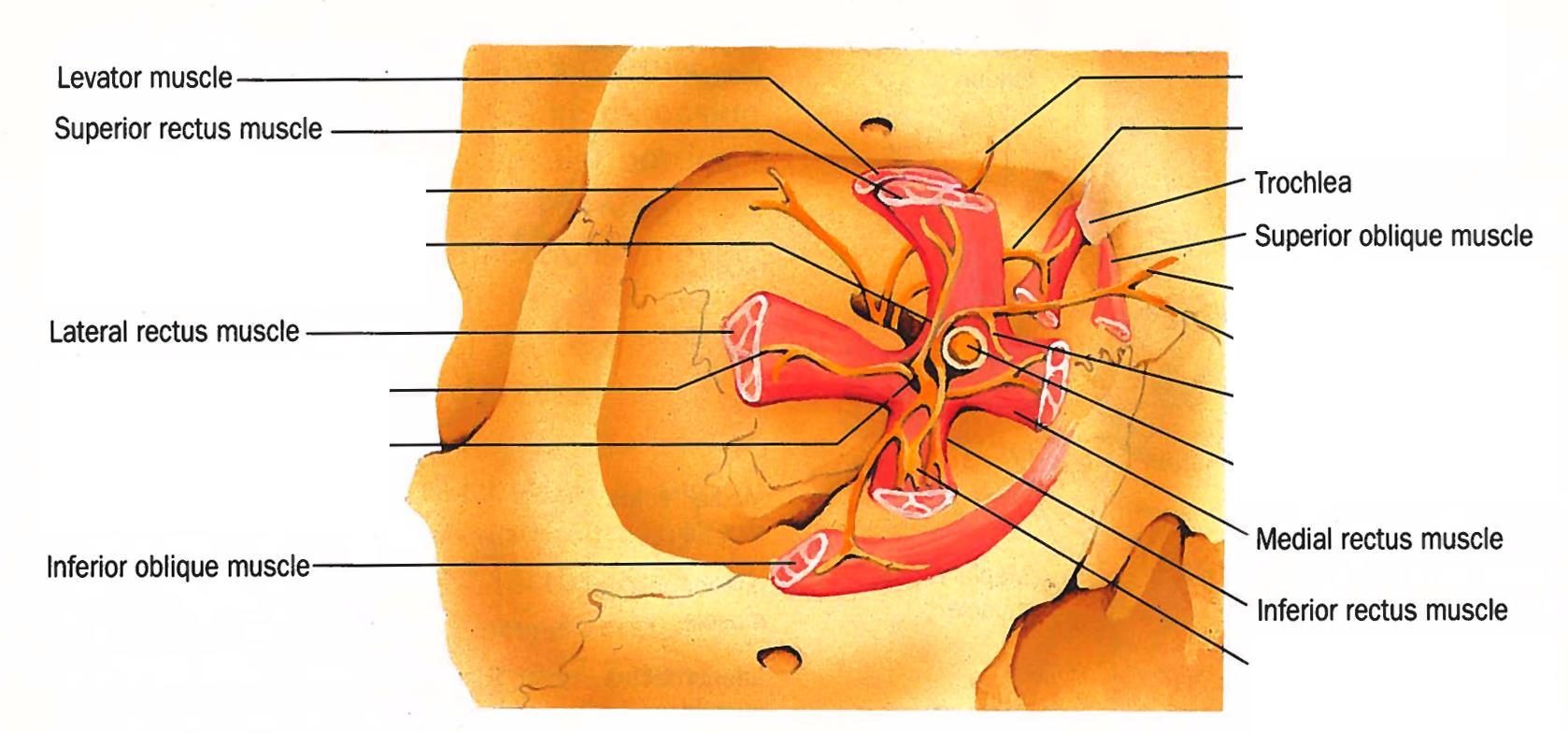
Orbit, right eye, demonstrating the extraocular muscle insertions.
The four rectus muscles originate from the tendinous ring called the Annulus of Zinn, which lies just anterior to the superior orbital fissure which is straddled by the greater and lesser wings of the sphenoid bone. The superior oblique muscle arises from the periosteum of the body of the sphenoid bone. The inferior oblique muscle arises from the medial orbital floor adjacent to the lacrimal fossa. The levator palpebrae superioris originates from the lesser wing of the sphenoid bone.
Image credit: American Academy of Ophthalmology. Modified and used with permission for educational purposes.
Extraocular Muscle
Medial rectus
Inferior rectus
Lateral rectus
Superior rectus
Superior oblique
Inferior oblique
Levator palpebrae superioris
Origin
Annulus of Zinn
Annulus of Zinn
Annulus of Zinn
Annulus of Zinn
Periosteum of sphenoid bone, above/medial to optic foramen
Maxillary bone (orbital floor) lateral to lacrimal fossa
Lesser wing of sphenoid bone superior to annulus of Zinn
Here are a few take-home points:
The rectus muscles originate from the annulus of Zinn.
The superior oblique and levator palpebrae superioris muscles originate from the sphenoid bone.
The Superior oblique muscle originates from the body of the Sphenoid bone.
The Levator palpebrae superioris originates from the Lesser wing.
The inferior oblique muscle arises from the orbital floor just lateral to the lacrimal fossa, which empties into the nasolacrimal duct.
Extraocular Muscle Insertions
The Spiral of Tillaux
The 4 rectus muscles do not insert at the same distance from the limbus; the medial rectus inserts closest to the limbus, with the inferior rectus, lateral rectus, and superior rectus muscles progressively inserting farther away, resulting in an imaginary spiral termed the spiral of Tillaux.
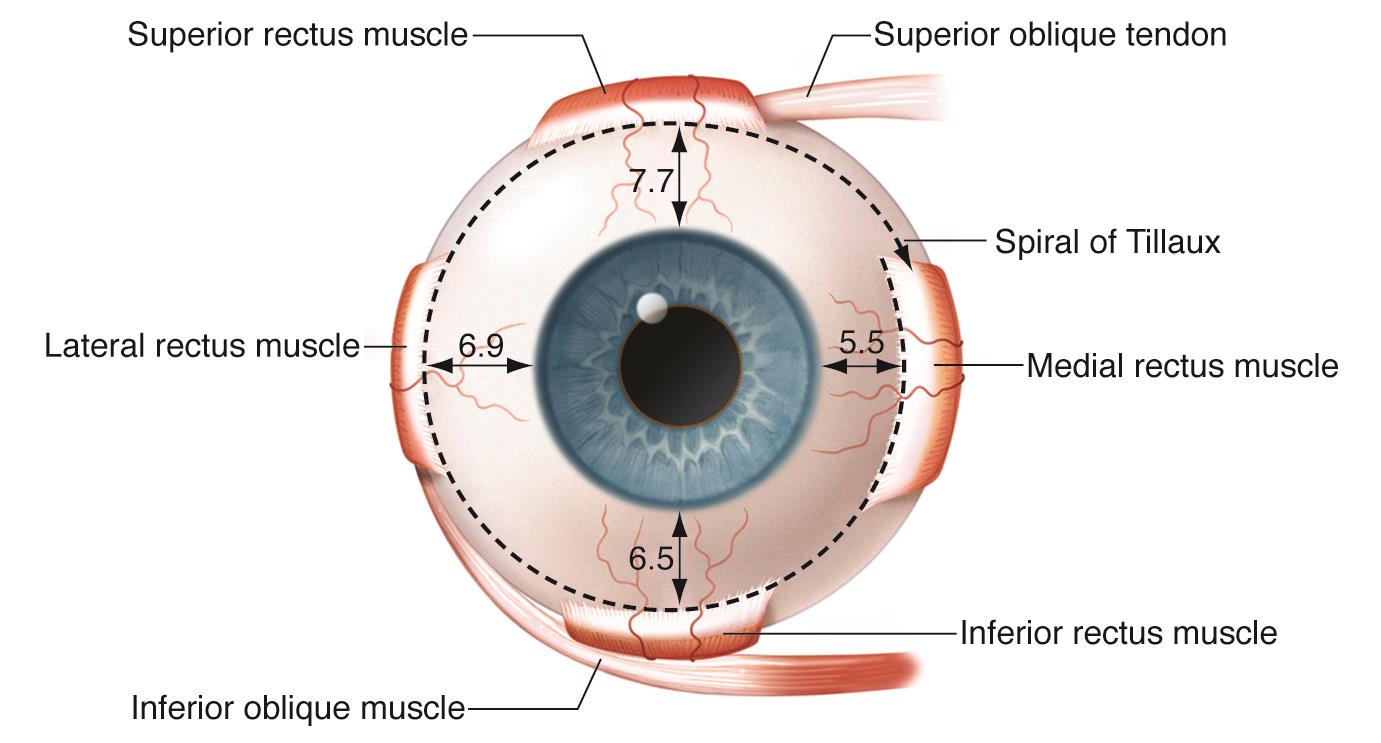
Spiral of Tillaux, right eye.
Note that the insertion distances, given in millimeters, are maximum values. Insertion distances vary in individuals.
Image credit: Illustration by Christine Gralapp. American Academy of Ophthalmology. Used with permission for educational purposes.
Here the values expressed in a table format:
Rectus Muscle
Medial rectus
Inferior rectus
Lateral rectus
Superior rectus
Distance From Limbus To Insertion
5.5 mm
6.5 mm
6.9 mm
7.7 mm
Clinical Significance
These measurements need to be memorized because of surgical considerations:
Knowing these measurements are important when performing any surgery involving the conjunctiva, sclera, or extraocular muscles. Some examples include:
Glaucoma surgeries (especially tubes and trabeculectomies)
Scleral surgeries
Retinal surgeries (especially scleral buckle surgery)
Trauma repair (extraocular muscle exploration, scleral exploration)
Strabismus surgeries
Because the ora serrata (the boundary between the retina and pars plana of the ciliary body) lies between 5.75 mm (nasal) and 6.50 mm (temporal) posterior to Schwalbe line (which conceptually forms the anterior-most border of the limbus), sutures passing too deeply at or behind the extraocular muscle insertions are at risk for perforating the retina, resulting in retinal holes and tears.
Extraocular Muscle Trivia
Medial Rectus
The medial rectus is the only rectus muscle that does not have an oblique muscle running tangential to it.
There is no point of reference for finding the muscle if it is lost/slipped.
Of the rectus muscles, the medial rectus has shortest tendon (4.5 mm); the inferior oblique muscle has the shortest tendon overall (1 mm).
Lateral Rectus
Of the rectus muscles, the lateral rectus has the broadest arc of contact (12 mm); the inferior oblique muscle has the broadest arc of contact overall (15 mm).
The lateral rectus muscle is the only extraocular muscle supplied by the lacrimal artery (also receives supply from the lateral/superior muscular branch of the ophthalmic artery).
The lateral rectus muscle is connected to the inferior oblique muscle by a frenulum of the intermuscular septum.
This must be disconnected with lateral rectus muscle surgery or the inferior oblique muscle may be inadvertently advanced with. the lateral rectus muscle.
The lateral rectus muscle is the thinnest extraocular muscle (9.2 mm wide).
Superior Rectus
The superior rectus muscle is loosely attached to the levator palpebrae superioris muscle.
When the eye is hypotropic, a pseudoptosis may be present because the upper eyelid will follow the superior rectus muscle.
With resection of the superior rectus muscle, the eyelid may be pulled downward (typically is not retracted upward with recessions).
The superior rectus muscle is connected to the superior oblique muscle by a frenulum of the intermuscular septum.
Inferior Rectus
Along with the inferior oblique muscle, the inferior rectus muscle receives partial arterial supply from the infraorbital artery (also receives supply from the medial/inferior muscular branch of the ophthalmic artery).
The inferior rectus muscle is strongly attached to the lower eyelid retractors.
Recession of the inferior rectus muscle results in lower eyelid retraction (eyelid moves down).
Resection of the inferior rectus muscle results in lower lid narrowing (eyelid moves up).
Superior Oblique
The superior oblique muscle has the longest tendon of all the extraocular muscles (26 mm).
The functional origin of the superior oblique tendon is the trochlea (though the muscle itself arises from the periosteum of the sphenoid bone body), which redirects the superior oblique to allow for its primary action of incyclotorsion.
The superior oblique muscle is connected to the superior rectus muscle by a frenulum of the intermuscular septum.
Inferior Oblique
The inferior oblique muscle has the shortest tendon of all the extraocular muscles (0-1 mm).
The inferior oblique muscle has the shortest muscle of all the extraocular muscles (37 mm).
Along with the inferior rectus muscle, the inferior oblique muscle receives partial supply from the infraorbital artery (also receives supply from the medial/inferior muscular branch of the ophthalmic artery).
The inferior oblique muscle insertion overlies the macula; surgical procedures should take care to minimize prolonged cautery over the insertion.
Surgery on the lateral portion of the inferior oblique where it crosses the inferior rectus muscle may injure the nerve supplying the inferior oblique muscle as well as pupillomotor preganglionic parasympathetic nerves, which can result in a dilated pupil.
The inferior oblique muscle may have more than one belly (10% have 2 bellies, rarely there can be 3 bellies); surgery on the inferior oblique muscle should explore for additional bellies to prevent ineffective surgery.
The inferior oblique muscle is connected to the lateral rectus muscle by a frenulum of the intermuscular septum.
Extraocular Muscle Orientation
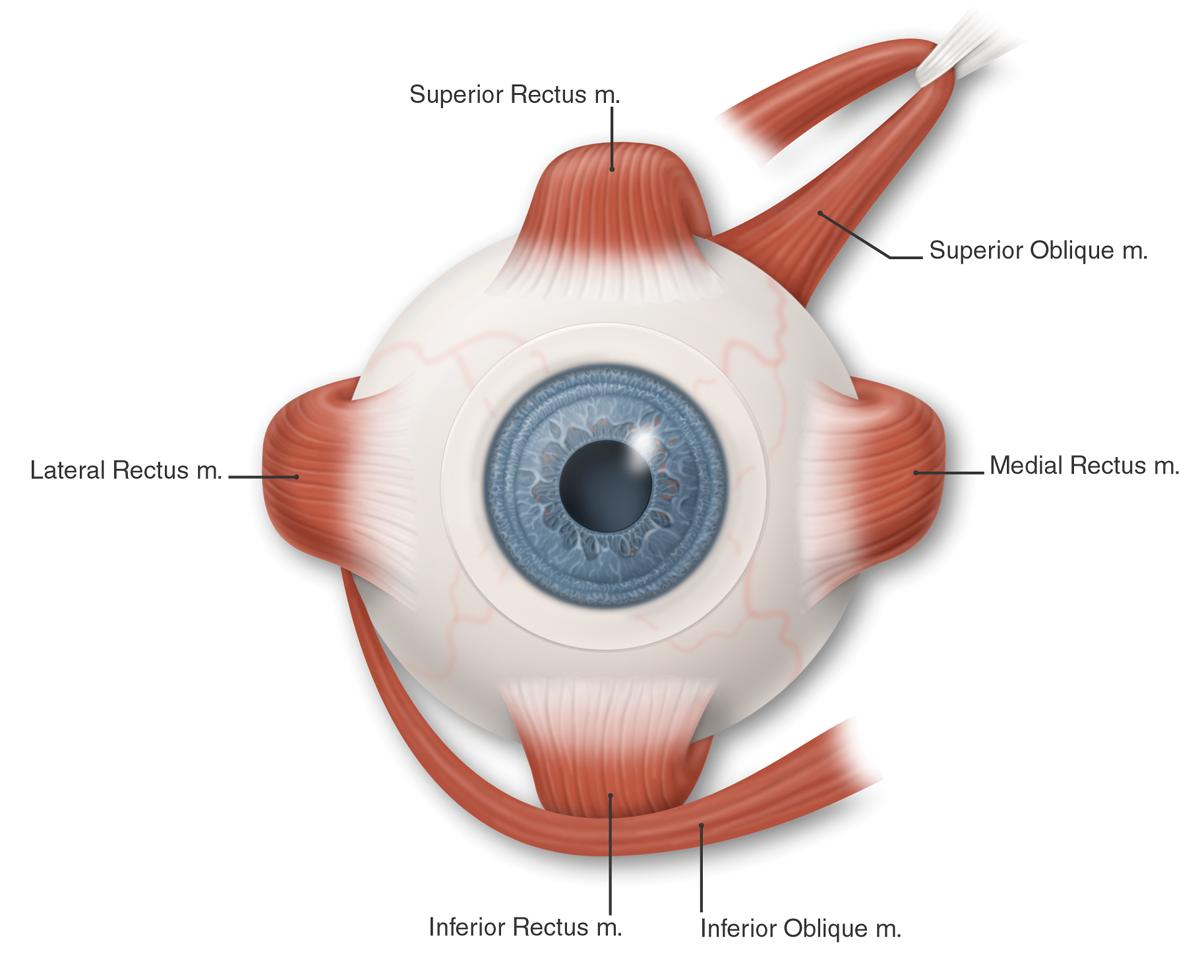
Image credit: American Academy of Ophthalmology. Used with permission for educational purposes.
The oblique muscles pass underneath their corresponding rectus muscles (superior oblique runs underneath the superior rectus, the inferior oblique runs underneath the inferior rectus).
The oblique muscles course across the globe to insert laterally.
Extraocular Muscle Actions
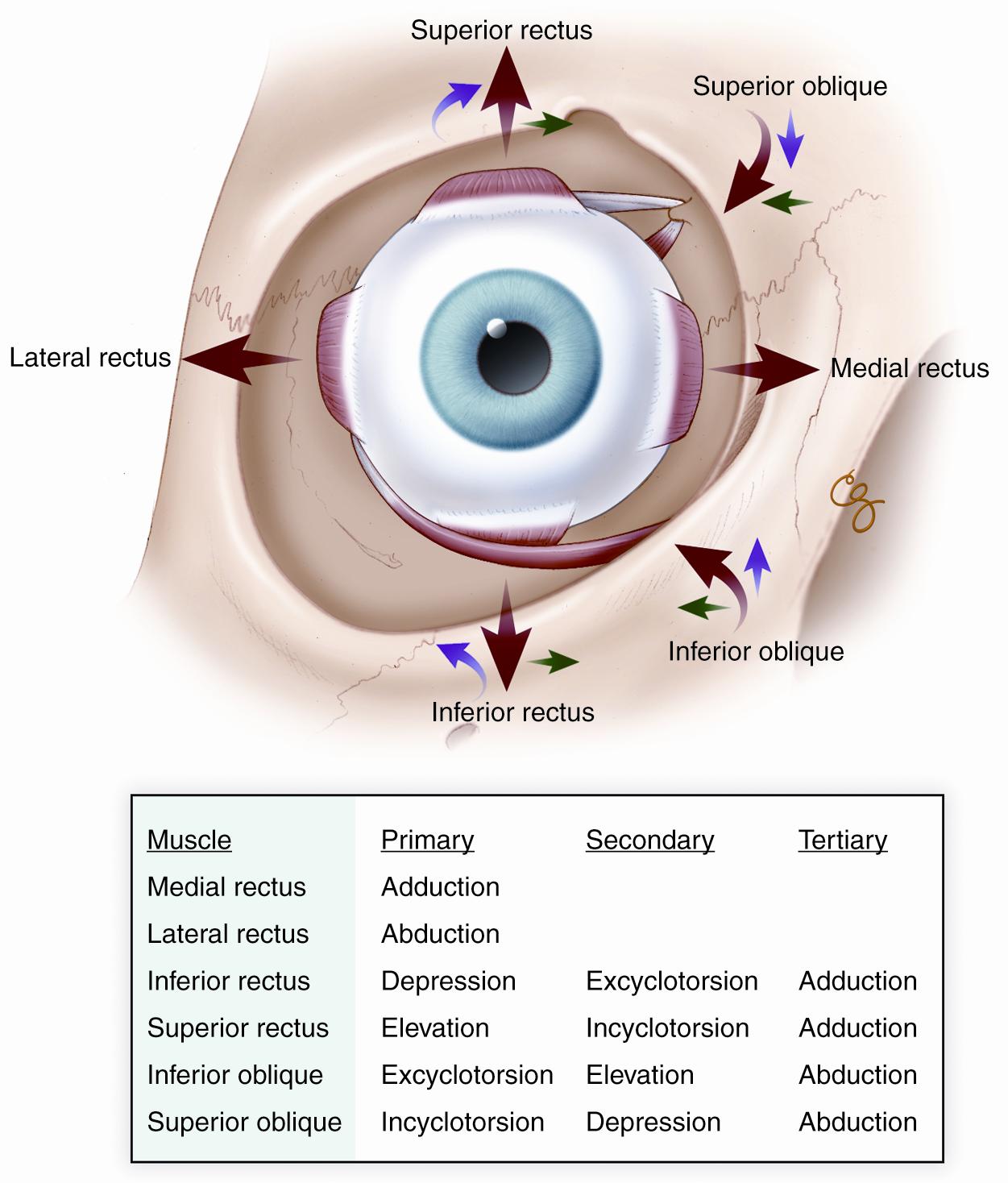
Image credit: Illustration by Christine Gralapp. American Academy of Ophthalmology. Used with permission for educational purposes.
Here are a few take-home points and helpful hints:
Excyclotorsion is seen in superior oblique/CN IV palsy because there is unopposed contraction of the inferior oblique.
The oblique muscles abduct the eye (“abduction is an oblique crime”).
The inferior muscles (inferior rectus and inferior oblique muscles) excyclotort the eye (“extortion is an inferior crime”)
Depending on the horizontal position of the eye (adducted or abducted), the primary action of the vertical muscles may change:
For example, in adduction the inferior oblique is the primary elevator of the eye and the superior oblique is the primary depressor; in abduction the superior rectus is the primary elevator and the inferior rectus muscle is the depressor.
Motility diagrams reflect this relationship between the various actions of the extraocular muscles:

Cardinal positions of gaze. Motility diagrams are typically drawn to reflect the actions of the extraocular muscles in the cardinal positions.
Image credit: American Academy of Ophthalmology. Used with permission for educational purposes.
Extraocular Muscle Arterial Supply
The arterial supply for the extraocular muscles primarily comes from branches of the ophthalmic artery:
Muscular branches: these form the anterior ciliary arteries that enter the eye to connect with the major arterial circle of the ciliary body.
Superior/inferior (BCSC Fundamentals book)
Medial/Lateral (BCSC Pediatrics book)
Lateral muscular branch: supplies the lateral rectus, superior rectus, superior oblique, and levator palpebrae superioris muscles
Medial muscular branch: supplies inferior rectus, medial rectus, and inferior oblique muscles
Lacrimal artery: partially supplies lateral rectus muscle
There is some partial supply of the inferior oblique and inferior rectus muscles from the infraorbital artery, a branch of the maxillary artery (from the external carotid artery circulation).
Extraocular Muscle Innervation
CN III (oculomotor nerve) innervates the following extraocular muscles:
Superior rectus
Medial rectus
Inferior rectus
Inferior oblique
Levator palpebrae superioris
CN IV (trochlear nerve) supplies the superior oblique muscle.
Keep in mind that CN IV passes above the annulus of Zinn and does not run within the muscle cone. Retrobulbar anesthesia does not affect CN IV, and by implication, does not paralyze the superior oblique muscle.
CN VI (abducens nerve) supplies the lateral rectus muscle.
Extraocular Muscle Structure
Introductory Concepts
Extraocular muscles need fast-twitch fibers to allow for saccades.
Extraocular muscles need to maintain sustained contraction with resistance to fatigue to allow for gaze fixation and vergence movements.
Extraocular muscles need finely-tuned “tonic” fibers that allow for slow contraction in smooth pursuit movements.
Extraocular muscles appear to be directly affected by the surrounding connective tissue, which form a fibroelastic pulley system that help the muscles maintain stable positions within the orbit and ensure that contraction of those muscles results in the desired action. While the pulley system’s significance is not completely understood, it is thought that abnormalities of this pulley system may result in various types of strabismus.
Organization
There are two basic types of muscle fibers:
Tonic-type muscle fibers: unique to extraocular muscles, they contract slowly and smoothly.
They are associated with smooth pursuit eye movements.
The fibers are innervated by multiple grapelike nerve endings (en grappe).
Twitch-type muscle fibers: similar to skeletal muscle fibers, they contract rapidly.
They are associated with rapid saccadic eye movements.
The fibers are innervated by platelike nerve endings (en plaque).
These muscle fibers are singly innervated.
There are two layers of extraocular muscles:
There is an outer (superficial) orbital layer that attaches to the connective pulley system.
There is an inner (deep) global layer that attaches to the globe itself.
Innervation
There is a very high ratio of nerve fibers to muscle fibers (1:3-1:5); this allows for very finely-tuned and precise eye movements.
A large percentage (80% of the orbital layer, 90% of the global layer) of extraocular muscle fibers are singly-innervated; this means that the muscle fiber has its own nerve axon (most striated muscle fibers may be bundled together so that one nerve axon activates hundreds of muscle fibers).
Singly-innervated muscle fibers are fast-twitch and are resistant to fatigue.
Singly-innervated orbital layer muscle fibers are considered the major contributor to sustained extraocular contraction. For this reason, damaging the motor nerves or end plates (such as with botulinum toxin) preferentially affects these fibers the most.
References
Basic and Clinical Science Course, Section 2. Fundamentals and Principles of Ophthalmology. American Academy of Ophthalmology. San Francisco: 2018-2019 edition, 11-12.
Basic and Clinical Science Course, Section 6. Pediatric Ophthalmology and Strabismus. American Academy of Ophthalmology. San Francisco: 2018-2019 edition, 19-30.