I admit, this one may be a bit more ambitious than is possible to cover in the span of just one article. Obviously, there are TONS of medications, many of them with very vague side effects. Throughout your career you will most likely see many people referred by another doctor for an eye exam because they were placed on a medication that listed "blurred vision" or "eye problem" as a side effect. Your patients may ask you about this. You also may prescribe some medications that need systemic monitoring. While the OKAP probably won't quiz you over some obscure side effect of some uncommonly used medication, there are definitely some ophthalmic and systemic side effects that we need to know very well. While I will try to discuss the salient points in a coherent manner, detailed information will have to be addressed in other articles. This article will also have overlapping information with the Fundamentals section.
As a disclaimer, there are far more adverse effects out there than the ones I'm listing here in this article. Since this is a review article, I'm trying to account for the more common and more likely-to-be-tested conditions; so it's very possible that adverse reactions I didn't list here will show up on testing or in practice questions.
Causes of Bone Marrow Toxicity
- Nafcillin
- Cefoxitin
- Pentamidine
- Chloramphenicol
- Amphotericin B
- Ganciclovir/Valganciclovir
Exacerbation of Myasthenia Gravis
- Telithromycin
- Ciprofloxacin (systemic)
- Statins
Increased Intracranial Pressure*
- Tetracyclines
- Vitamin A derivatives
*There are a lot of medications that have been implicated in the presentation of papilledema and increased intracranial pressure, some with more support than others. Because many of the medications listed (such as cyclosporine, oral contraceptives, fluoroquinolones, etc.) are very rarely implicated in increased intracranial pressure, I have left them off the review list. The papilledema and intracranial pressure typically resolves with discontinuation of the medication. Because this is a secondary cause for intracranial hypertension, the terms idiopathic intracranial hypertension and pseudotumor cerebri should not be used to described these conditions (since the cause is no longer "idiopathic").
Antibiotics
Penicillins
- Penicillin allergy is the most common antibiotic allergy (3-5% in the general population, 10% in patients with previous exposure to penicillin).
Cephalosporins
- Cephalosporin and penicillin cross-sensitivity is well known. Approximately 10% of people with penicillin allergies will also be allergic to cephalosporins.
- Cefoxitin (Mefoxin) can induce bone marrow and liver toxicity.
- Cefotetan (Cefotan) can cause hemolytic anemia, or a disulfiram-like reaction with alcohol intake.
Aminoglycosides
- Systemic administration of aminoglycosides can cause kidney damage (nephrotoxicity) and hearing loss (ototoxicity).
- Subconjunctival and intravitreal injections of aminoglycosides have an increased risk of retinal ischemia. Gentamicin is more likely to cause retinal ischemia than amikacin or tobramycin.
Fluoroquinolones

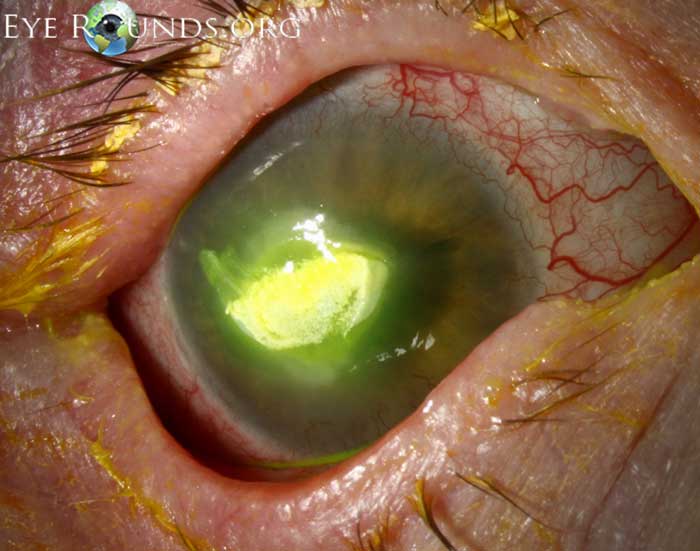
Ciprofloxacin corneal deposits.
Image credit: University of Iowa, EyeRounds.org.
- Prolonged topical ciprofloxacin leads to white corneal deposits and corneal toxicity. These deposits will resolve with discontinuation of the medication. Later-generation fluoroquinolones do not share this feature.
Sulfonamides
- Sulfa medications have been known to cause Stevens-Johnson syndrome, which can affect the conjunctiva.
Tetracyclines
- Tetracyclines are contraindicated in pregnancy and in children < 10 years old, as they can deposit in teeth and bones.
Chloramphenicol
- Chloramphenicol has been reported to cause optic atrophy.
- There is an idiosyncratic and fatal aplastic anemia that can occur with chloramphenicol. It is irreversible.
Antifungals
Amphotericin B
- Systemic use of amphotericin B can cause all sorts of bad side effects (hence the nickname "amphoterrible"). It can lead to thrombophlebitis, nephrotoxicity, hypokalemia, bone marrow suppression, and cardiotoxicity.
Antivirals
Foscarnet
- Foscarnet can cause nephrotoxicity.
Cidofovir
- Cidofovir has been associated with anterior uveitis in up to 37% of patients.
Antihypertensives
β-blockers
- β-blockers can cause bronchospasm, decrease heart rate, mask hypoglycemia, increase serum triglycerides, and decrease exercise tolerance.
Antiepileptics
Topiramate (Topamax)
- Topiramate can cause secondary angle-closure glaucoma with acute myopia as a result of ciliary body swelling.
Sample Questions (answers at the bottom of the page)
1. A patient with HIV presents with the fundus finding on the right. What test should be used to monitor systemic antiviral treatment to avoid adverse side effects?
A. Liver profile
B. Complete blood count
C. CD4 count
D. Serum creatinine
2. What aspect of the history is most important to the evaluation of the clinical findings on the right?
A. Nocturnal hypertension
B. Recent fever
C. Acne
D. Family history of vision loss
3. A 72-year-old man presents 5 days after cataract surgery with increased redness, decreased vision, and eye pain. The slit lamp exam is shown on the right. What is the LEAST optimal intravitreal treatment?
A. Ceftazidime
B. Vancomycin
C. Ceftriaxone
D. Amikacin



{kind=link}
Sample Question Answers
- B. CMV retinitis is treated with a combination of antivirals (ganciclovir or valganciclovir) and HAART. Because systemic ganciclovir can cause myelotoxicity, intravitreal ganciclovir is recommended. If systemic ganciclovir is used, a complete blood count can monitor for myelotoxicity. While some HAART medications can affect the liver, the question is specifically directed towards treatment with ganciclovir. Image from: asrs.org.
- C. Optic nerve swelling can be secondary to many conditions, including papilledema, nonarteritic anterior ischemic optic neuropathy, and anterior optic neuritis. A history of nocturnal HYPOtension is helpful in considering nonarteritic anterior ischemic optic neuropathy. A recent history of fevers is nonspecific, and while it may suggest a viral prodrome prior to optic neuritis or a systemic inflammation such as giant cell arteritis, it could also be completely unrelated to the condition. A history of acne is important to ascertain, as several acne treatments (isoretinoin, tetracyclines) are implicated in increased intracranial pressure. A family history of vision loss is helpful in Leber's hereditary optic neuropathy, but the optic nerve is rarely (if ever) swollen to the degree seen in the image. This patient had a history of minocycline use. Image from: University of Michigan.
- D. Ceftazidime and vancomycin are standard treatments for endophthalmitis. Ceftriaxone is typically not used in the initial intravitreal treatment of endophthalmitis. Amikacin is an aminoglycoside and may carry an increased risk of retinal ischemia when injected intravitreally or subconjunctivally. Image from: ejournalofophthalmology.com.
{kind=link}
{kind=link}
References and Additional Reading
- Basic and Clinical Science Course, Section 1: Update on General Medicine. American Academy of Ophthalmology, 2017-2018 edition.
- Basic and Clinical Science Course, Section 2: Fundamentals and Principles of Ophthalmology. American Academy of Ophthalmology, 2017-2018 edition.
Do you have any suggestions on what else might be important to remember about medications that may show up on the OKAP? Do you have any tips for helping to remember all of this information? Do you have any requests for specific topics to cover? Leave a comment or contact us!