
To help increase the amount of helpful study content on this site, I’ve partnered with some medical students from East Tennessee State University! They are being mentored by one of my former ophthalmology residents, Dr. Brent Aebi. The posts are primarily authored by the medical student, and reviewed/edited by myself and Dr. Aebi.
This post about thyroid eye disease was written by Zachary Shelton, B.S.
Thyroid eye disease (TED), also known as Graves ophthalmopathy or thyroid-associated orbitopathy, is an autoimmune inflammatory disorder of the orbit characterized by enlargement of extraocular muscles, expansion of orbital fat, and secondary effects on the eyelids, ocular surface, and optic nerve. (1, 2) Although most commonly associated with Graves disease, TED may also occur in euthyroid or hypothyroid patients, including those with Hashimoto thyroiditis, demonstrating that the autoimmune mechanisms underlying orbital inflammation are distinct from thyroid hormone status alone. (1, 2)
Thyroid eye disease is classically described as following a biphasic course, progressing from an active inflammatory phase to a stable fibrotic phase, a concept often illustrated by Rundle’s curve. (3) However, longitudinal data suggest that the disease course is more variable. (2, 3) Periods of stability do not always represent permanent dormancy, as reactivation or smoldering inflammation can occur, sometimes years after initial resolution. (5, 12) Although uncommon, reactivation has been reported even after prolonged stability and may be associated with triggers such as periocular surgery. (5)Recognizing this evolution is central to understanding the clinical trajectory of thyroid eye disease, which should be viewed as dynamic and individualized rather than strictly biphasic. (5, 12)
Epidemiology and Risk Factors (2, 3, 11, 12)
TED is the most common cause of orbital disease and exophthalmos in adults
Occurs more frequently in women, though the disease is often more severe in men
Peak incidence occurs in middle adulthood
The disease shows a unimodal age distribution, with peak incidence occurring between ages 50 and 59
It is more common in women, although men are more likely to develop severe forms
Prevalence varies by race and ethnicity, with the highest rates reported in Black individuals (0.12%), followed by White (0.11%), Asian (0.07%), and Hispanic (0.05%) populations
Approximately 90 percent of patients have Graves disease, though ocular disease may precede or follow thyroid dysfunction
MAJOR RISK FACTORS
Cigarette smoking, which increases the severity and prolongs the active phase
Family history of thyroid disease
Thyroid-stimulating immunoglobulin positivity
Radioactive iodine therapy without steroid prophylaxis
Higher total cholesterol and LDL levels have been observed in patients with thyroid eye disease and may be associated with an increased risk
Smoking is the strongest modifiable risk factor and is associated with poorer response to therapy.
Pathophysiology
TED is driven by autoimmune activation of orbital fibroblasts expressing thyroid-stimulating hormone receptors and insulin-like growth factor 1 receptors. (4, 8) These fibroblasts proliferate and differentiate into adipocytes and myofibroblasts, producing excess glycosaminoglycans. (4)
The result is:
· Tissue edema
· Extraocular muscle enlargement
· Orbital fat expansion within a rigid bony cavity (4, 8)
Over time, inflammation subsides, and fibrosis replaces edema, leading to permanent structural changes. (2, 4) This transition explains why early disease responds to immunomodulatory therapy, while late disease is dominated by mechanical restriction.
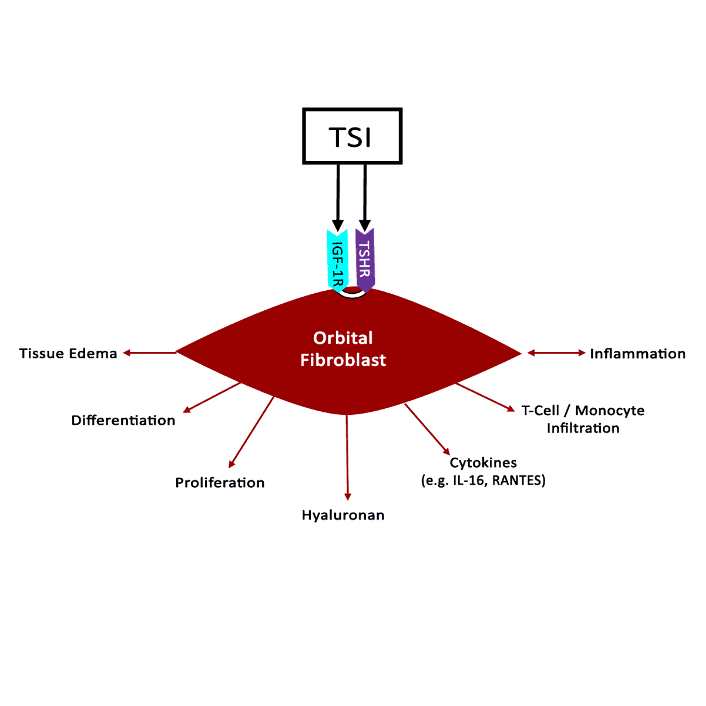
Image credit: University of Iowa. https://webeye.ophth.uiowa.edu/eyeforum/tutorials/thyroid-eye-disease/index.htm#gsc.tab=0

Image credit: University of Iowa. https://webeye.ophth.uiowa.edu/eyeforum/tutorials/thyroid-eye-disease/index.htm#gsc.tab=0
Disease Course
ACTIVE INFLAMMATORY PHASE (2, 7)
Orbital pain or pressure
Eyelid edema and erythema
Conjunctival injection and chemosis
Fluctuating diplopia
Progressive proptosis
Traditionally, this phase has been described to last one year in nonsmokers and may persist two to three years in smokers. (2, 12)
INACTIVE FIBROTIC PHASE (2, 7)
Minimal inflammatory signs
Stable eyelid retraction
Fixed proptosis
Restrictive strabismus due to muscle fibrosis
At this stage, medical anti-inflammatory therapy has limited benefit.
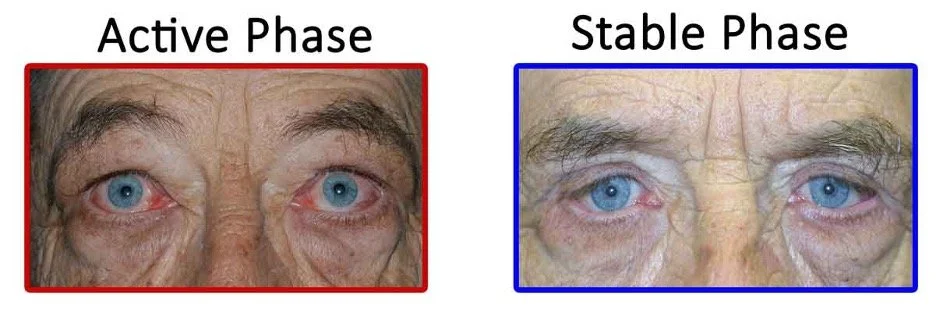
Image credit: University of Iowa (EyeRounds). https://eyerounds.org/patients/thyroid-eye-disease.htm
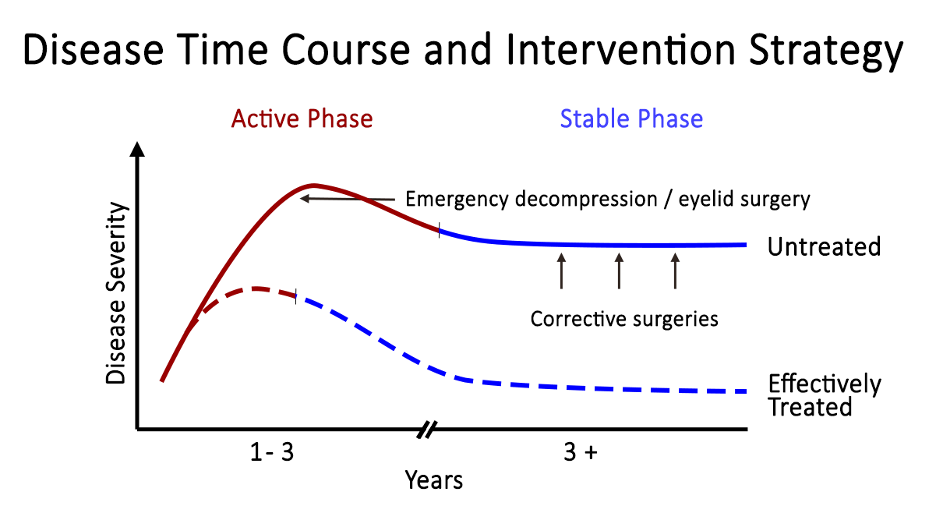
Image credit: University of Iowa (EyeRounds). https://eyerounds.org/patients/thyroid-eye-disease.htm

Note the periorbital edema, eyelid retraction, scleral show, and conjunctival injection.
Image credit: University of Iowa. https://webeye.ophth.uiowa.edu/eyeforum/tutorials/thyroid-eye-disease/index.htm#gsc.tab=0
Image credit: University of Iowa. https://webeye.ophth.uiowa.edu/eyeforum/tutorials/thyroid-eye-disease/index.htm#gsc.tab=0
Eyelid and Ocular Surface Findings (2, 4, 6)
Eyelid retraction is the most common and often the earliest clinical sign.
TYPICAL FINDINGS
Upper eyelid retraction
Lid lag
Temporal flare
Increased palpebral fissure height
CONSEQUENCES OF EXPOSURE
Dry eye symptoms
Foreign body sensation
Photophobia
Exposure keratopathy
Corneal epithelial breakdown and ulceration in severe cases
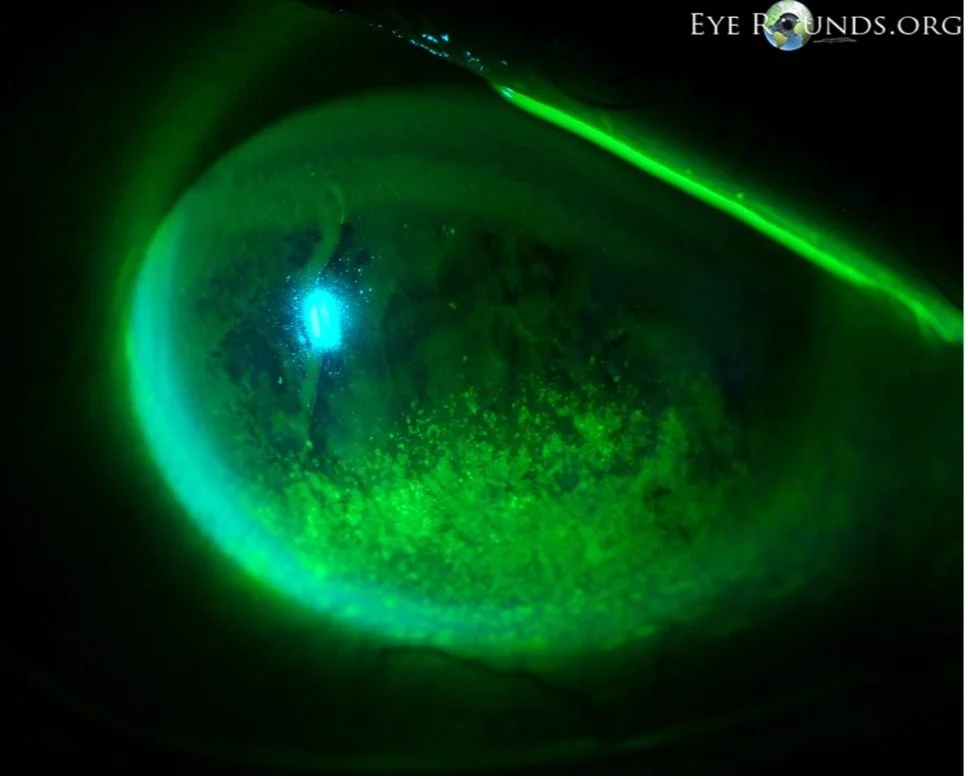
Exposure keratopathy. Punctate epithelial erosions (PEE) secondary to exposure keratopathy.
Image credit: University of Iowa. https://webeye.ophth.uiowa.edu/eyeforum/tutorials/thyroid-eye-disease/index.htm#gsc.tab=0
Extraocular Muscle Involvement
Extraocular muscle inflammation progresses to fibrosis, producing mechanical restriction rather than neurogenic paresis.
FREQUENCY of Involvement (1)
Inferior rectus
Medial rectus
Superior rectus–levator complex
Lateral rectus
Oblique muscles
Mnemonic for frequency of Involvement
“I’M SLO(w)”
*Remember, this refers to the relative FREQUENCY of extraocular muscle involvement, NOT the order of presentation.
Clinical consequences include vertical diplopia and limited elevation. Forced duction testing is positive.
*Clinical and board exam pearl: Many TED patients will have diplopia patterns that mimic cranial nerve palsies or myasthenia gravis. Positive forced ductions (demonstrating muscle restriction) help differentiate TED from these other causes.
Proptosis and Orbital Congestion (1, 5, 8)
Proptosis and orbital congestion can progress to major displacement of the globe. If severe enough, an exposed cornea may thin or perforate due to severe dryness, and compression or traction on the optic nerve may cause irreversible damage. The degree of proptosis does not reliably predict disease severity or optic nerve risk. In rare cases, proptosis combined with a shallow orbit can cause globe subluxation, which warrants immediate action.
Proptosis results from:
Extraocular muscle enlargement
Orbital fat expansion
Increased orbital pressure
Associated findings:
Conjunctival chemosis
Episcleral venous congestion
Elevated intraocular pressure, particularly in upgaze
Increased intraocular pressure in upgaze results from inferior rectus restriction combined with impaired episcleral venous outflow.

Image credit: University of Iowa (EyeRounds). https://eyerounds.org/patients/thyroid-eye-disease.htm
Dysthyroid Optic Neuropathy (6, 8)
Compression of the optic nerve at the orbital apex by enlarged extraocular muscles leads to dysthyroid optic neuropathy. Failure to decompress the optic nerve quickly may result in permanent vision loss. (*Board question pearl)
CLINICAL FEATURES
Decreased visual acuity
Dyschromatopsia, often preceding acuity loss
Any pattern of visual field defects
Relative afferent pupillary defect
Optic disc edema may be present early, while optic atrophy late
Diagnosing Thyroid Eye Disease
Diagnosis is primarily clinical. Though there are several autoimmune markers that are associated with autoimmune thyroid disease, these are not currently required for the diagnosis of TED. (1) Key diagnostic elements:
Eyelid retraction and lid lag
Proptosis
Restrictive diplopia
Ocular surface disease
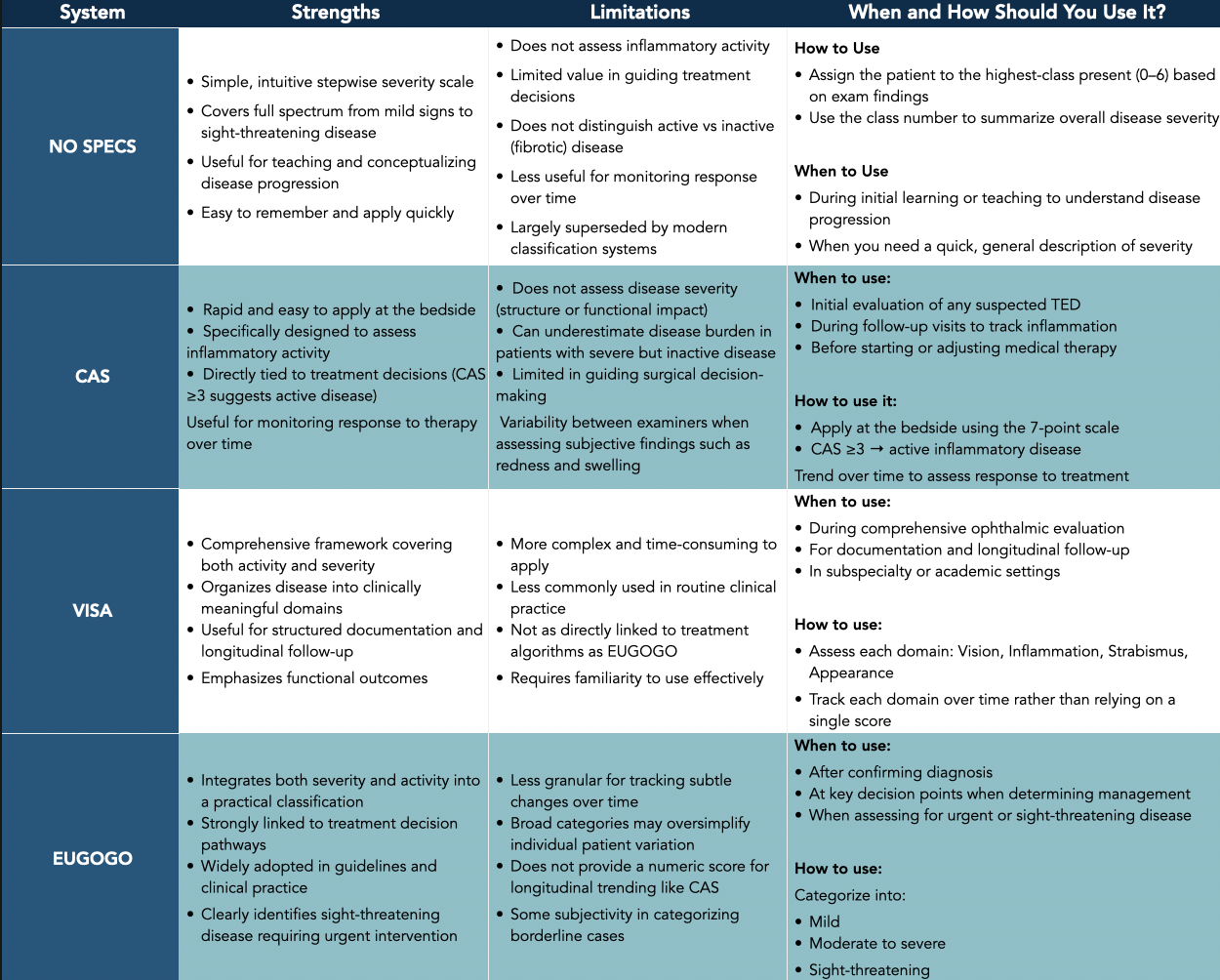
Assessing Activity and Severity (1, 2, 5, 7)
NO SPECS, CAS, VISA, and EUGOGO frameworks
Thyroid eye disease is assessed using complementary scoring systems that describe inflammatory activity, disease severity, and functional impact. No single system captures all dimensions of the disease. Instead, NO SPECS, CAS, VISA, and EUGOGO each emphasize different aspects of the TED spectrum and are often used together to guide management.
NO SPECS
NO SPECS provides a stepwise grading of disease severity from minimal findings to sight-threatening complications, but it does not account for inflammatory activity and therefore has limited utility in guiding modern management.
NO SPECS Components
· Class 0: No signs or symptoms
· Class 1: Only signs
· Class 2: Soft tissue involvement
· Class 3: Proptosis
· Class 4: Extraocular muscle involvement
· Class 5: Corneal involvement
· Class 6: Sight loss
CLINICAL ACTIVITY SCORE (CAS)
Measuring Inflammatory Activity
The Clinical Activity Score is designed to quantify ongoing orbital inflammation. It focuses on signs and symptoms that reflect active, potentially reversible disease rather than fixed anatomic changes.
CAS Components
One point is assigned for each of the following:
Spontaneous orbital pain
Pain with eye movement
Eyelid erythema
Eyelid edema
Conjunctival injection
Chemosis
Caruncle or plica inflammation
Interpretation
CAS ≥ 3 at initial evaluation suggests active inflammatory disease
CAS ≥ 4 on follow-up indicates persistent activity
CAS is independent of disease severity. Patients with pronounced proptosis or diplopia may have a low CAS if disease is inactive, while others with minimal structural changes may have a high CAS during active inflammation.
CAS is particularly valuable when followed over time, as declining scores often parallel resolution of inflammation even when fibrotic sequelae persist.
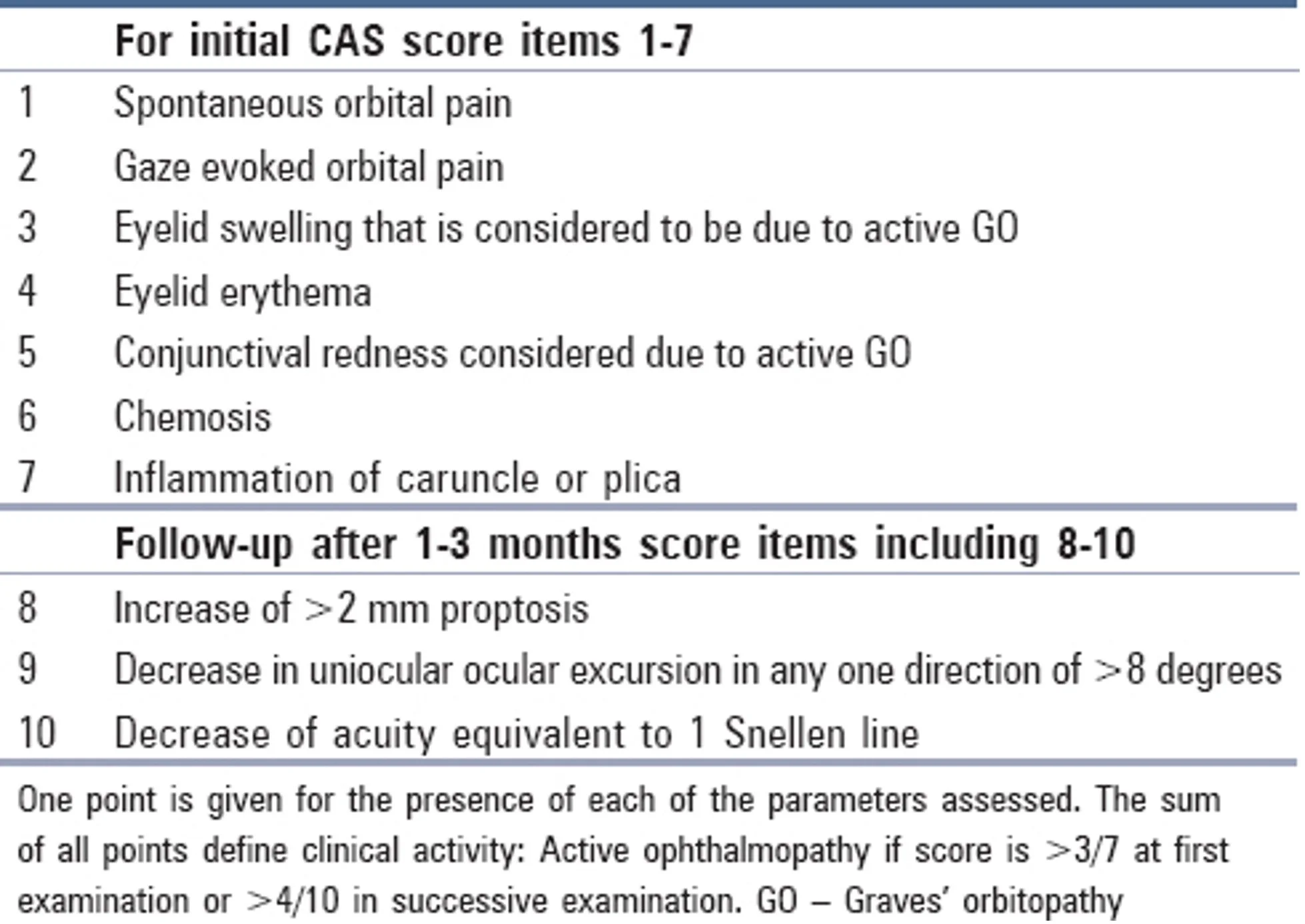
Image credit: American Academy of Ophthalmology (EyeWiki). https://eyewiki.org/Thyroid_Eye_Disease#Grading
VISA CLASSIFICATION
The VISA system was developed to provide a broader clinical framework that incorporates both disease activity and functional consequences. It organizes findings into four domains:
V — Vision: optic nerve function, visual acuity, color vision, visual fields
I — Inflammation: pain, redness, swelling, chemosis
S — Strabismus: diplopia and motility restriction
A — Appearance: eyelid retraction, proptosis, cosmetic impact
VISA emphasizes that thyroid eye disease affects vision, motility, and appearance in parallel, and that these domains may evolve independently over time. It is particularly useful for comprehensive documentation and longitudinal follow-up.
EUGOGO CLASSIFICATION
The European Group on Graves’ Orbitopathy (EUGOGO) classification is widely used to guide treatment decisions by stratifying disease according to severity rather than inflammatory activity alone.
EUGOGO Severity Categories
Mild disease
Minor lid retraction
Mild soft tissue involvement
No or intermittent diplopia
Minimal impact on daily life
Moderate to severe disease
Marked soft tissue involvement
Significant proptosis
Constant or functionally limiting diplopia
Sight-threatening disease
Dysthyroid optic neuropathy
Severe exposure keratopathy
EUGOGO categories align closely with management pathways, distinguishing patients who may be managed conservatively from those requiring immunomodulatory therapy or urgent intervention.
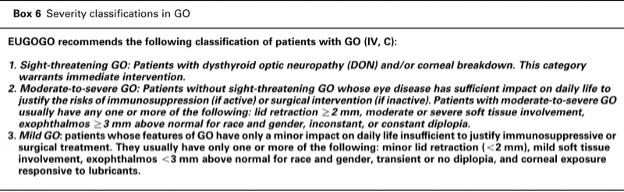
Image credit: American Academy of Ophthalmology (EyeWiki). https://eyewiki.org/File:EUGOGO_Classification.png
Imaging Integration (1, 8, 9)
Hallmark imaging finding
Fusiform enlargement of extraocular muscle bellies with relative tendon sparing (*Board questions pearl)
Additional findings:
Orbital fat expansion
Forward globe displacement
Optic nerve stretching
MRI helps distinguish active inflammatory edema from fibrotic disease. CT is particularly useful for evaluating apical crowding and surgical planning.
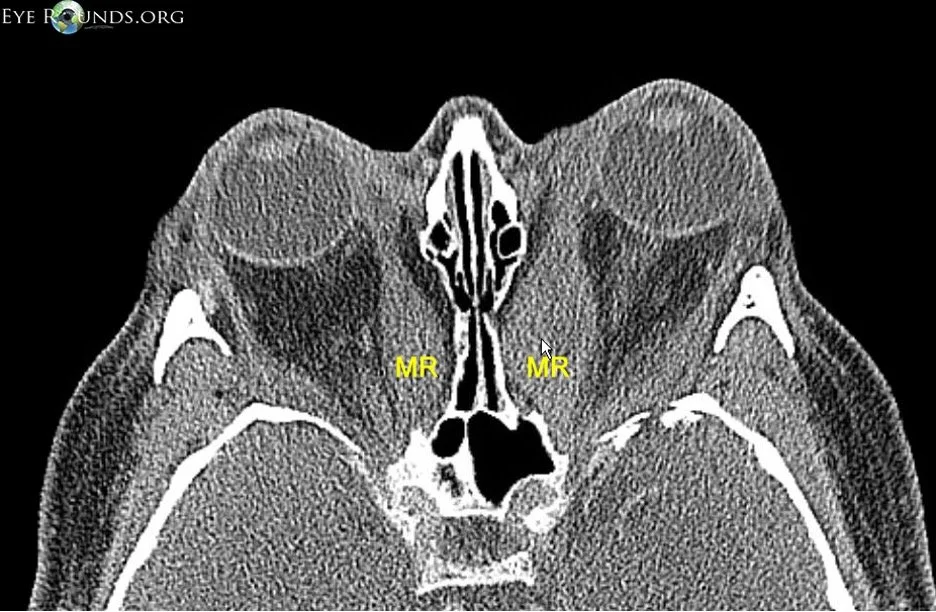
Axial CT scan showing enlarged muscle belly in Thyroid Eye Disease. The medial rectus muscle is marked "MR."
Image credit: University of Iowa. https://webeye.ophth.uiowa.edu/eyeforum/atlas/pages/Thyroid-Eye/index.htm#gsc.tab=0
{kind=link}
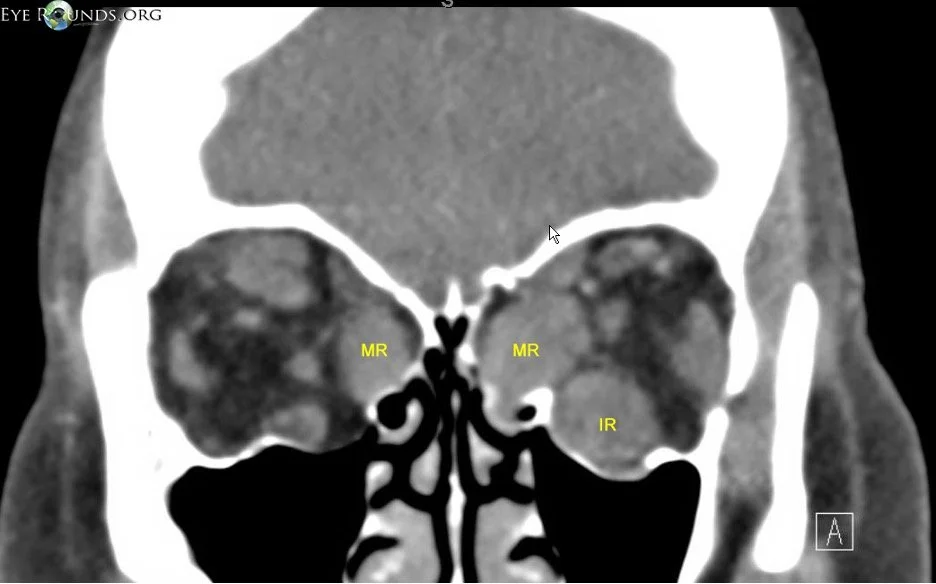
Coronal CT scan showing the enlarged muscle bellies in cross-section. The medial rectus muscle is marked "MR" and the inferior rectus is labeled "IR."
Image credit: University of Iowa. https://webeye.ophth.uiowa.edu/eyeforum/atlas/pages/Thyroid-Eye/index.htm#gsc.tab=0
Identifying Vision-Threatening Disease on Imaging
Critical features include:
Apical crowding of enlarged extraocular muscles
Optic nerve straightening
Effacement of surrounding cerebrospinal fluid spaces
Severe optic nerve compression may occur even in patients with minimal proptosis.
Management Principles (1, 5, 7)
Across all presentations, treatment requires a calibrated approach, sufficiently aggressive to protect vision while minimizing long-term treatment-related toxicity.
CONSERVATIVE CARE
Appropriate for all patients and often sufficient for mild or inactive disease.
Smoking cessation and maintenance of euthyroid status reduce disease severity and duration
Ocular surface protection with lubrication, moisture chambers, eyelid taping, or tarsorrhaphy when needed
Temporary relief of diplopia with prisms or occlusion
Selenium supplementation for selected patients with mild, noninflammatory disease
MEDICAL THERAPY
Generally reserved for active inflammatory disease.
Systemic corticosteroids to reduce orbital inflammation, limited by systemic toxicity
Teprotumumab, an insulin-like growth factor 1 receptor inhibitor, significantly reduces inflammation and proptosis and is the first FDA-approved therapy for thyroid eye disease. Other similar medications are currently under investigation, with veligrotug being approved by the FDA in June 2026.
Other immunomodulatory agents may be considered in refractory cases
ADJUNCTIVE THERAPY
Low-dose orbital radiation is an adjunct in active disease, particularly for motility restriction
SURGICAL MANAGEMENT
Reserved for inactive disease or vision-threatening complications.
Orbital decompression when indicated
Strabismus surgery after decompression and stabilization
Eyelid repositioning once ocular alignment is stable
References
EyeWiki. (n.d.). Thyroid eye disease. American Academy of Ophthalmology. https://eyewiki.org/Thyroid_Eye_Disease
Shah, S. S., Stokkermans, T. J., & Patel, B. C. (2025). Thyroid eye disease. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK582134/
American Academy of Ophthalmology. (n.d.). What is Graves disease? American Academy of Ophthalmology. https://www.aao.org/eye-health/diseases/what-is-graves-disease
Bahn, R. S. (2010). Graves’ ophthalmopathy. New England Journal of Medicine, 362(8), 726–738. https://doi.org/10.1056/NEJMra0905750
Bothun, E. D., Scheurer, R. A., & Lee, M. S. (2009). Update on thyroid eye disease and management. Clinical Ophthalmology, 3, 543–551. https://pmc.ncbi.nlm.nih.gov/articles/PMC2770865/
EyeWiki. Dysthyroid optic neuropathy. American Academy of Ophthalmology. Accessed May 20, 2026. https://eyewiki.org/Dysthyroid_Optic_Neuropathy
Liaboe, C. A., Simmons, B. A., Clark, T. J., & Shriver, E. M. (n.d.). Thyroid eye disease. EyeRounds, University of Iowa. https://eyerounds.org/patients/thyroid-eye-disease.htm
University of Iowa, Department of Ophthalmology & Visual Sciences. (n.d.). Thyroid eye disease tutorial. EyeRounds. https://webeye.ophth.uiowa.edu/eyeforum/tutorials/thyroid-eye-disease/index.htm
University of Iowa Department of Ophthalmology & Visual Sciences. Thyroid eye disease atlas. EyeRounds.org. https://webeye.ophth.uiowa.edu/eyeforum/atlas/pages/Thyroid-Eye/index.htm#gsc.tab=0
University of Michigan Health. (n.d.). Thyroid eye disease (TED or Graves eye disease). https://www.uofmhealth.org/our-care/specialties-services/thyroid-eye-disease-ted-or-graves-eye-disease
Vincent, A. B., Engelmann, A. R., Hwang, C. J., & Nasr, C. (2025). Thyroid eye disease: What’s the latest? Cleveland Clinic Journal of Medicine, 92(11), 693–701. https://doi.org/10.3949/ccjm.92a.25043
Wiersinga, W. M. (2025). Natural history of Graves’ orbitopathy. In W. M. Wiersinga & G. J. Kahaly (Eds.), Graves’ orbitopathy: A multidisciplinary approach (pp. XX–XX). Springer. https://doi.org/10.1007/978-3-031-99672-6_2